Sprache
Sprache Türkçe
Türkçe English
English Arabic
Arabic Germany
Germany Russian
RussianHand osteoid osteoma: evaluation of diagnosis and treatment

Abstract
Background: OO
(osteoid osteoma) is a common, osteoblastic, benign bone tumor but rarely seen
in the hand region. There is still some debate about the diagnosis and
treatment of hand OOs. In the present study, we aimed to evaluate the
epidemiology, radiologic features, surgical treatment options and functional
outcomes.
Methods: Between
January 2003 and December 2014, surgically treated and pathologically verifed 9
hand OO cases were investigated retrospectively. The preoperative and
postoperative clinical outcome scores were calculated using the M2-DASH
(Manchester-Modifed Disabilities of Arm Shoulder and Hand) Score.
Results: Lesion
locations were as follows: middle phalanx in 2/9 (22%) patients (2nd and 4th
digit), proximal phalanx in 6/9 (67%) patients (one 4th, two 2nd and three 5th
digits) and metacarpal (2nd) in 1/9 (11%) patient. Incidence of nidus formation
was 6/9 (67%) on X-ray, 7/9 (78%) on CT imaging and 2/9 (22%) on MR imaging.
The mean time to diagnosis was 13.22±5.44 months. Preoperative mean M2-DASH
score was 41±6 and postoperative was 7.4±8.6.
Conclusion: Osteoid
osteoma is usually seen below 25 years, and rarely found over 40 years of age.
There is male dominance with a male to female ratio of 3:1. Delay of diagnosis
may be encountered because of many diferential diagnoses. When OO is suspected,
CT imaging should be taken before the MR imaging. Because of superiority in
soft tissue imaging, MR imaging should be an alternative tool in complex cases.
Keywords: Hand,
Metacarpal, Osteoid, Osteoma, Phalangea
Background
Osteoid osteoma (OO) is a vascularized,
osteogenic, benign bone tumor and was frst defned by Heine in 1927 [1] and frst
described by Jafe in 1935 [2]. Te lesion is characterized as a well-defned
lytic area with the vas[1]cularized
central nidus which is surrounded by sclero[1]sis and cortical thickening
in X-ray and computerized tomography (CT) imaging. Magnetic resonance (MR)
imaging usually shows an extensive bone marrow and/ or soft tissue edema [3–5].
OO is rarely seen in the hand region. Delay of diagnosis can be experienced,
because of diferent clinical, radiological and histological features from the
long bone OOs [6, 7]. Further, diferential diag[1]nosis and nonspecifc
fndings on radiographs complicate the diagnosis. Most of the papers are case
reports, but still, there is a need for case series due to the rarity and
difculties in diagnosing. In the present study, we aimed to evaluate the
epidemiology, radiologic features, surgical treatment options and functional
outcomes
Methods
Te study was performed in accordance
with the ethical standards of the Declaration of Helsinki. All patients
provided informed consent before inclusion in the study, and a local ethics
committee approved the study protocol. Tis study was performed on sur[1]gically
treated 9 hand OO patients from January 2003 to December 2014. Inclusion
criteria were histologi[1]cally
verifed metacarpal and phalangeal OO. Patients who had previous percutaneous or
surgical treatment and patients with recurrence were excluded from the study.
All patients were evaluated regarding swell[1]ing, pain, trauma history,
night pain, response to pain relievers, duration of complaints and time to
diagnosis. All patients were evaluated with X-ray, CT, MR and SPECT-CT
imaging preoperatively. Te preoperative and postoperative clinical outcome
scores were cal[1]culated
using the M2-DASH (Manchester-Modifed Disabilities of Arm Shoulder and Hand)
Score [8]. Sta[1]tistical
analysis was performed using SPSS software (IBM, Armonk, NY) using an unpaired
Student’s t test and the Fisher exact test. Statistical signifcance level was
set at p ≤ .05.
Results
Seven (78%) of patients were male, and 2
(22%) were female, and the mean age was 29±7 years. Lesion loca[1]tions
were as follows: proximal phalanx in 6/9 (67%

patients (one 4th, two 2nd and three 5th
digits), middle phalanx in 2/9 (22%) patients (2nd and fourth digit), and
metacarpal (2nd) in 1/9 (11%) patient. Te mean time to diagnosis was
13.22±5.44 months. Tere were night pain, localized swelling, tenderness
and response to pain relievers in all patients. Also, there were slight
erythema[1]tous
changes and local skin temperature increase in 3/9 (33%) patients. Complete
blood count, erythrocyte sedi[1]mentation
rate and C-reactive protein (CRP) levels were normal in all patients. Incidence
of nidus formation was 6/9 (67%) on X-ray, 7/9 (78%) on CT imaging and 2/9
(22%) on MR imaging. Cortical thickening rate was 7/9 (78%) on X-ray, 7/9 (78%)
on CT imaging and 3/9 (33%) on MR imaging. Non-specifc fndings were found in 2/9
(22%) cases both on X-ray and CT imaging. Bone and/ or soft tissue edema rate
was 8/9 (89%) on MR imaging (Table 1). All except one were treated by
unroofng and curettage using “Burr-down” method. En bloc resection was
performed in one case (11%). Mean M2-DASH score was 41±6 and improved to
7.4±8.6 postoperatively. Complications were seen in 4/9 (44%) patients. During
a mean of 43.44±16.58 months of follow-up, case num[1]ber 1 required a second
intervention because of residual tumor, after 6 months from the curettage
(Fig. 1). Tis residual tumor was treated successfully with radiofre[1]quency
treatment. Despite the rehabilitation protocol, 30° proximal interphalangeal
joint fexion persisted in this patient. Case 2 has encountered a superfcial
infec[1]tion
which was treated with oral antibiotics. In cases 7 and 9, temporary superfcial
wound problems were

encountered, which did not require
treatment. No other complication was encountered (Table 2)
Discussion
Tis study aimed to evaluate the
epidemiology, radio[1]logic
features, surgical treatment options and functional outcomes. Male:female ratio
was 3:1 in our series. Gen[1]der
ratio in this present study adds a diferent ratio to the literature. But this
diferent data may be related to small patient numbers. Variable male:female
ratios were reported, but similarly with this present study there is a
signifcant male predominance in literature [6, 9–11]. In our series, mean age
was in the third decade. In the literature, OOs are usually seen below the
fourth decade, reported in the second or third decade, and most patients
are<25 years old [9]. Phalanges were the most commonly afected bone and
the most common involvement was in proximal pha[1]langes. In addition,
metacarpal bone settlement was the most rare one in our study, with a rate of
1/9 (11%). Te most frequent location for OO in the hand region seems like
proximal phalanges. Ozdemir et al. reported settle[1]ment as 11 (60%) proximal
and 4 (20%) middle phalan[1]ges
in 18 cases [11]. Jafari et al. reported settlement as 10 (40%) proximal,
5 (20%) distal phalanges and only 4/25 (16%) metacarpal in 25 cases [9].
Incidence of nidus formation was 6/9 (67%) on X-ray and mean time to diagnosis
was 13.22±5.44 months in this study. Similarly, Jafari et al.
concluded that only 13 patients (52%) had the characteristic appearances of
oste[1]oid
osteoma on X-ray, and they reported that the average time from the onset of
symptom to successful treatment was 16.3±11.1 months [9]. On X-rays, nidus
formation may not be seen or may need to pass a long time to form [12].
Marcuzzi et al. reported that nidus incidence was 2/18 (11%) on X-ray.
Tey concluded that the initial radi[1]ographs
of almost all of the patients were normal. Also, they reported that the
classical appearance of the dis[1]ease
can only be observed between 6 and 25 months. If the nidus has enough time
to mature, it could be seen on X-ray [6]. However, we could not fnd additional
informa[1]tion
about their mean time to diagnosis. Te duration of maturation and its
pathogenesis are still unknown. Tus, initial X-ray examinations are often
normal. Tis fact may be related to transposition, lack of periosteal reac[1]tion
or cortical thickening. In the majority of our cases, nidus was detected on
direct radiographs, but surely both planes should be taken. Typical appearance
of nidus was mostly on anteroposterior and in lateral views only cor[1]tical
thickening was noted. Also, normal scintigraphic fndings may have been due to
low metabolic activity in a mature osteoid osteoma [6]. Hand OO patients may be
treated conservatively for extended periods. A large number of diferentiating
dis[1]eases
directs the surgeon to shoot MR imaging instead of CT imaging. Te diagnostic
rate of CT imaging was high in our series. In CT imaging, cortical thickening
obscured the nidus in only one patient. On the contrary, sclerosis may range
from mild-cancellous to extensive-periosteal, and may obscure the nidus [13].
Tis result may be due to our use of thin section CT imaging in our cases. As a
result, CT imaging reported as superior to X-ray and MR imaging in diagnosis,
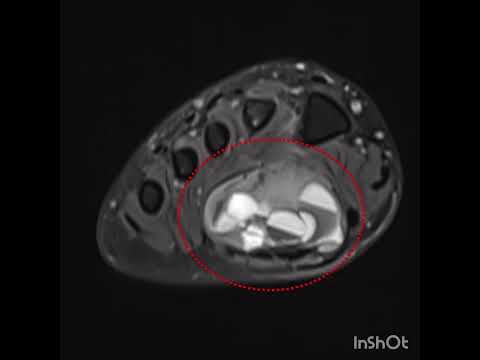
surgical planning and follow-up [9]. In MR imaging, nidus was detected in only
2 cases. Te remaining cases had bone and/or soft tissue edema which obscured
the nidus. MR imaging may depict the nidus and sclerosis because of adjacent
bone marrow and soft tissue edema [14, 15]. Bone and/or soft tissue edema was
seen on MR imaging, in all patients except one. Moreover, bone marrow and
soft-tissue edema, joint efusion, and synovitis are better appreciated at MR
imaging than at CT imaging [16]. Difuse bone and/ or soft tissue edema observed
on MR imaging [17] may shift the diagnosis and long-term immobilization may
be

suggested. In our case series mean
diagnostic time was similar to Jordan et al.’s systematic review [17]. Te
long[1]est
time to diagnose was 2 years due to nonspecifc fnd[1]ings in X-ray and CT
imaging. Te reason for the delay was generalized edema due to pregnancy that
hides the isolated fnger edema. After the regression of postpartum edema,
isolated fnger swelling got attention. It should be noted that the prolongation
of the treatment period causes social, economic, and psychological damage [18].
Pain was the most common symptom and all of our patients experienced night
pain. In all patients, the pain was partially relieved with painkillers. In
literature, the most common symptom is pain in hand OO [6, 9]. Pain severity
increases at night and responds to prostaglandin inhibitors [19, 20]. Jafari
et al. reported night pain rate as 21/25 (84%) and partial pain relief
rate as 17/25 (68%); Marcuzzi et al. reported partial pain relief as 8/18
(44%) [6, 9]. Tus, our results regarding the night pain and pain relief are not
compatible with the literature, and this shows that larger series are needed.
Te second common symptom has been reported as swelling [6, 9]. Swelling may be
related to the rich vascular supply or perme[1]ability, results from the
prostaglandins [21]. If OO settles near the joint, swelling and erythema
misdirect the sur[1]geon
to a diagnosis of arthritis. Many surgical techniques like en bloc resection,
corti[1]cal
peeling or burr-down with curettage, percutaneous curettage and alcoholization,
laser coagulation, ther[1]moregulation
or radiofrequency ablation were defned [22–24]. En bloc resection requires bone
grafting, and hand region is narrow for the percutaneous techniques [24, 25].
Cortical peeling is technically more difcult, especially with thick sclerosis,
stripping of the cortex may not always be provided. Finding a cherry-red spot
without disruption of typical appearance is possible with high-speed rolling
burr. We performed the burr-down technique with curettage for all patients,
except one. In one patient, 6 months after, a residual lesion was encoun[1]tered
which was treated successfully with radiofrequency. Because of a narrow
surgical feld, en bloc resection was performed only in one patient. We suggest
burr-down method with high-speed burr and because of the low recurrence rate,
grafts are not needed. To the best of our knowledge, the most recent and most
extensive series is from the year 2013 with a num[1]ber of 25 cases [9].
Remaining papers are the mostly small number of case series or case reports. Te
rarity of hand OOs limits to report larger series. Retrospec[1]tive,
non-comparative manner and number of cases are the limitations, but the rarity
obstructs the condi[1]tions
for reporting a more extensive, prospective rand[1]omized-controlled series.
Tere is still a need for more series to build more extensive reviews and
evidence[1]based
medicine.
Conclusion
Osteoid osteoma usually seen below
25 years old, and rarely found over 40 years of age. Tere is male
domi[1]nance
with a male to female ratio of 3:1. Delay of diag[1]nosis may be encountered
because of many diferential diagnoses. Local and sole presence of
non-traumatic, prolonged swelling, pain responding to painkillers, ten[1]derness,
erythema, and sclerosis which is consistent with pain should remind the OO.
When OO is suspected, CT imaging should be taken before the MR imaging. It
should be kept in mind that the diagnostic value of thin[1]section CT imaging is
higher than MR imaging. Because of superiority in soft tissue imaging, MR
imaging should be an alternative tool in complex cases. Unroofng and curettage
with “Burr-down” method seems to be efective in preventing residual tumors or
relapses.
Authors’ contributions
OE: conception or design of the work, data collection and data analysis with interpretation. VG: drafting the article, critical revision of the article and fnal approval of the version to be published. Both authors read and approved the fnal manuscript
Author details
Department of Orthopaedics, Haydarpasa Numune Training and Research Hospital, Health Sciences University, Tibbiye Cd No: 40 Uskudar, Istanbul, Turkey. 2 Department of Orthopaedics, Faculty of Medicine, Bezmialem Vakif University, Vatan Cd, Fatih, 34093 Istanbul, Turkey.
Acknowledgements
None.
The paper was presented as a poster/oral presentation at XVth National Congress of the Hand and Upper Extremity Surgery and 4th National Congress of the Hand Rehabilitation. May 11–15, 2016, Fethiye, Turkey.
Competing interests
The authors declare that they have no competing interests
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Consent for publication
Local consent was obtained for retrospective studies, and informed consent was taken from all patients participating in the study.
Ethics approval and consent to participate
All patients stated that full permission for the publication, reproduction, broadcast and other use of photographs, recordings, and other audio-visual material.